
Acute Injury Management (PEACE & LOVE)
- Samuel Stewart
- Feb 15
- 4 min read

I will briefly discuss acute injury management, and highlight that injury management philosophies and acronyms such as ICE, RICE, RICED are outdated and potentially detrimental to the recovery process regarding rest, ice and drugs (medications).
The acute injury management model proposed by Dubois & Esculier (2020) primarily draws on research on lateral ankle, muscular soft-tissue, and low back injuries but can be generalised to acute musculoskeletal injuries such as ACLs. The PEACE and LOVE acronyms proposed by Dubois & Esculier (2020) are shown in Figure 1.
Figure 1. PEACE and LOVE acronyms.
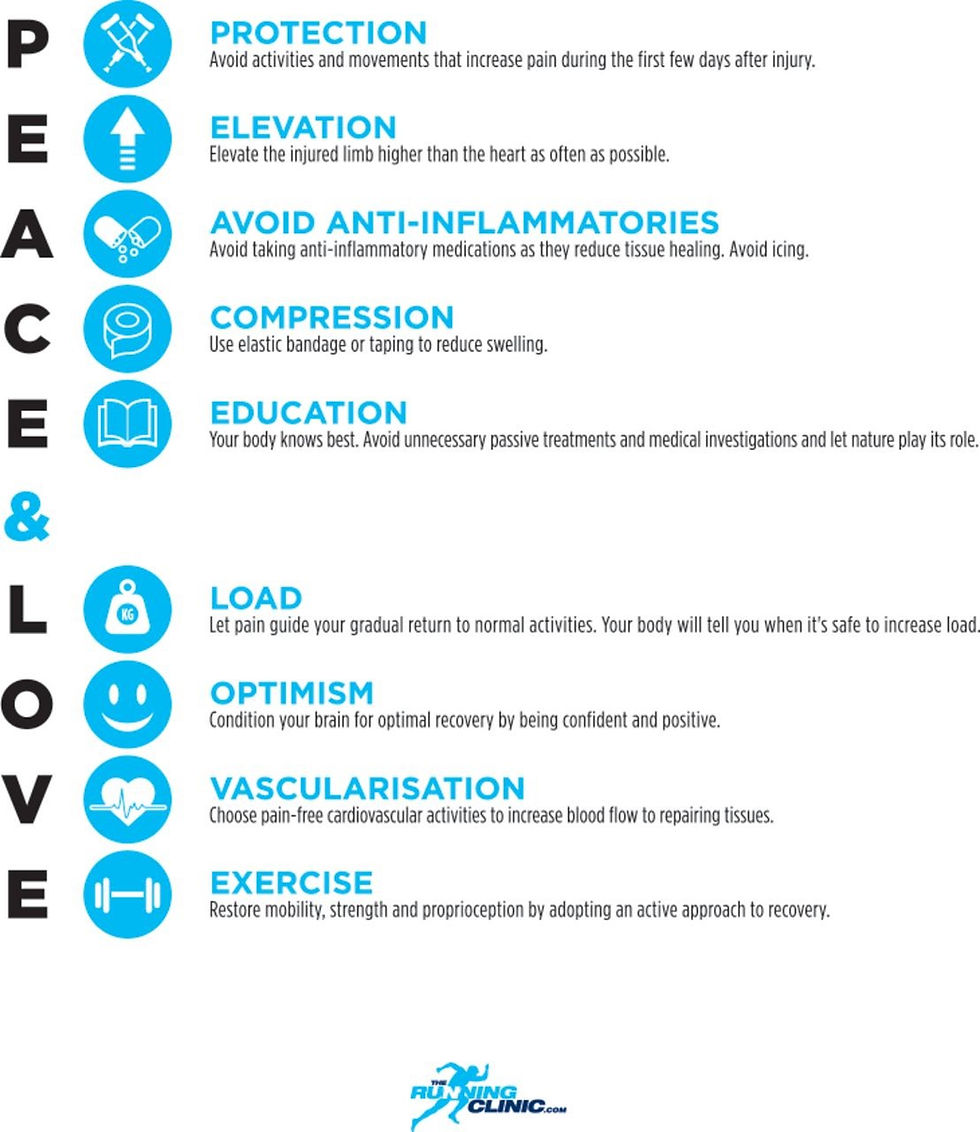
Note. From Dubois, B., & Esculier, J. F. (2020). Soft-tissue injuries simply need PEACE and LOVE. British journal of sports medicine, 54(2), 72–73. https://doi.org/10.1136/bjsports-2019-101253
Dubois & Esculier (2020) advocate for Protecting the injury and letting pain guide your activity, Elevating the injury above heart level when possible, Avoiding anti-inflammatories, Compression application or taping and Education to avoid unnecessary passive treatments and to choose pain-free activities to aid recovery (PEACE). Early movement is widely regarded as having multiple benefits and is encouraged for most injuries, which is why the ‘rest’ component of acute injury management is now challenged. McNair et al. (1996) observed that the 30% reduction in mean quadriceps torque after injecting fluid into the knee joint without producing pain could be restored by performing 3-4 minutes of submaximal exercise, which helped dissipate stress from the increased fluid volume. If active exercise is not possible or as an adjunct to exercise, Gatewood et al. (2017) found that neuromuscular electrical stimulation (NMES) improves quadriceps strength and overall knee functional outcomes for patients after arthroscopic knee surgery. Continued movement and participation in activities, as much as possible, without aggravating symptoms, is part of protection.

Knee joint swelling and pain are common symptoms following anterior cruciate ligament (ACL) injury (Cimino et al., 2010). Saline injections to simulate intra- or extra-articular swelling have been shown to cause knee pain and reduce muscle strength (Henriksen et al., 2011; Rice et al., 2014). Additionally, Henriksen et al. (2007) found that experimentally induced knee pain impaired knee joint control and stability during walking, potentially increasing the risk of knee injury. Furthermore, Loyd et al. (2019) found that reducing the peak postoperative swelling after total knee arthroplasty may lead to early improvements in quadriceps strength and functional recovery. Since persistent quadriceps weakness is common after ACL reconstruction (ACLR) (Krishan & Williams, 2011), early management of knee swelling could help reduce pain, aid restoration of quadriceps strength, protect the joint, reduce the degree of instability, and improve functional outcomes. Early loading or movement will likely aid in managing most, if not all, acute injuries by stimulating the lymphatic pump and promoting vascular return through muscular contraction, thereby providing a load that protects tissue from loss of capacity. Encouraging early and safe loading/movement is key to injury management.

Dubois & Esculier (2020) no longer include cryotherapy, which has previously been recommended for acute injury management (Bleakley et al., 2012). This change reflects Reinl's (2013) position that ice is a proinflammatory stimulus that impairs lymphatic fluid flow, which is essential for normal tissue recovery after injury. Along with Miranda et al. (2021), who concluded, based on two randomised controlled trials (RCTs), that there is a lack of high-quality evidence to support the use of cryotherapy for acute ankle injuries. The analgesic effects of cryotherapy may facilitate early mobilisation and movement, but they could also impair perception by altering input to the brain, thereby stimulating less appropriate pain output and compromising protective behaviours. Choosing to utilise cryotherapy is complex, as evidence of its harm is not as strong as Reinl (2013) suggests, but it presents a strong mechanistic case against its use. Additionally, it encourages passive behaviour over activity and movement. However, as with most clinical questions, the answer is most likely "it depends." There may be thresholds of swelling at which it becomes helpful to slow the clearance process, or combining modalities or specific injury types may yield different outcomes, such as muscle, tendon, musculotendinous junction, ligament, joint, or bone. Additionally, there is likely an interplay between what it helps and what it hinders. There is much we don’t know for certain, and some people may use the analgesic effect of cryotherapy to increase activity that may offset any negative physiological effects of cryotherapy if they would not otherwise have engaged in that activity.

The Dubois & Esculier (2020) model is the first to include taping within the compression component, reflecting increased utilisation of kinesiotaping (KT). A review by Hörmann et al. (2020) found some evidence for the efficacy of KT in treating postoperative oedema but acknowledged that all the reviewed trials were at high risk of bias and lacked a standard-care comparison. Balki et al. (2016) was one of the trials included by Hörmann et al. (2020), who found that KT application with muscle and lymphatic correction techniques in the acute phase after ACLR improved pain, swelling, knee flexion, and hamstring muscle strength. Exploring compression and KT use more broadly, Naci et al. (2020) compared compression stockings to KT in patients with chronic venous disease and observed that while both improved functional outcomes, oedema and pain were better controlled with compression. Compression, taping, and elevation are simple, flexible management strategies that can be adapted to patient preferences and environmental conditions to support recovery.

Therefore, general acute injury recommendations include participating in regular, pain-free movement to distribute pressure and fluid stress and to engage the lymphatic pump to move swelling. Elevate the injured area when possible, and avoid anti-inflammatory medications, given their potential to adversely affect tissue healing (Dubois & Esculier, 2020). Utilise regular compression wrapping, garments, or modalities, with or without KT application, as these can be used independently and may aid participation in increased movement and activities. While NMES is a passive modality, when utilised in conjunction with education on the importance of active participation in management, it may reduce swelling and restore muscle function, thereby supporting functional recovery. Other basic education concepts, such as hurt does not equal harm and movement and load can be safe and necessary, along with setting expectations early, are important parts of the management and recovery process.


Comments